Sigmoid Colon: Anatomy, Course, Functions, and 7 important clinical conditions
The sigmoid colon is also known as the pelvic colon due to its presence in the pelvic region. It is the last part of the large intestine nearest to the rectum and anus. It is the point where feces stays for a while before getting excreted. The sigmoid colon maintains a continuation from the descending colon to the rectum. It is usually present within the pelvis area. But, it often becomes displaced into the abdominal cavity due to its mobility.
The sigmoid colon is part of the hindgut. It receives its proper blood supply, nerve supply, and lymphatic drainage just like other parts of the hindgut. Normally, its diameter depends on the quantity of waste present in it. Its diameter is about one inch in the contracted state.
Anatomy of the sigmoid colon
The human gastrointestinal system is divided into three parts:
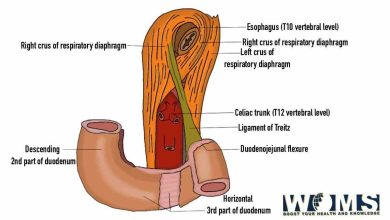
- Foregut – esophagus to the major duodenal papilla
- Midgut – major duodenal papilla to 2/3rd of transverse colon
- Hindgut – 2/3rd of the transverse colon to the rectum
The sigmoid colon is present in the region of the hindgut. The total length is about 25 to 40cm. It may offer several physiologic variants with greater length than normal. It is an S-shaped terminal portion of the large intestine.
Course
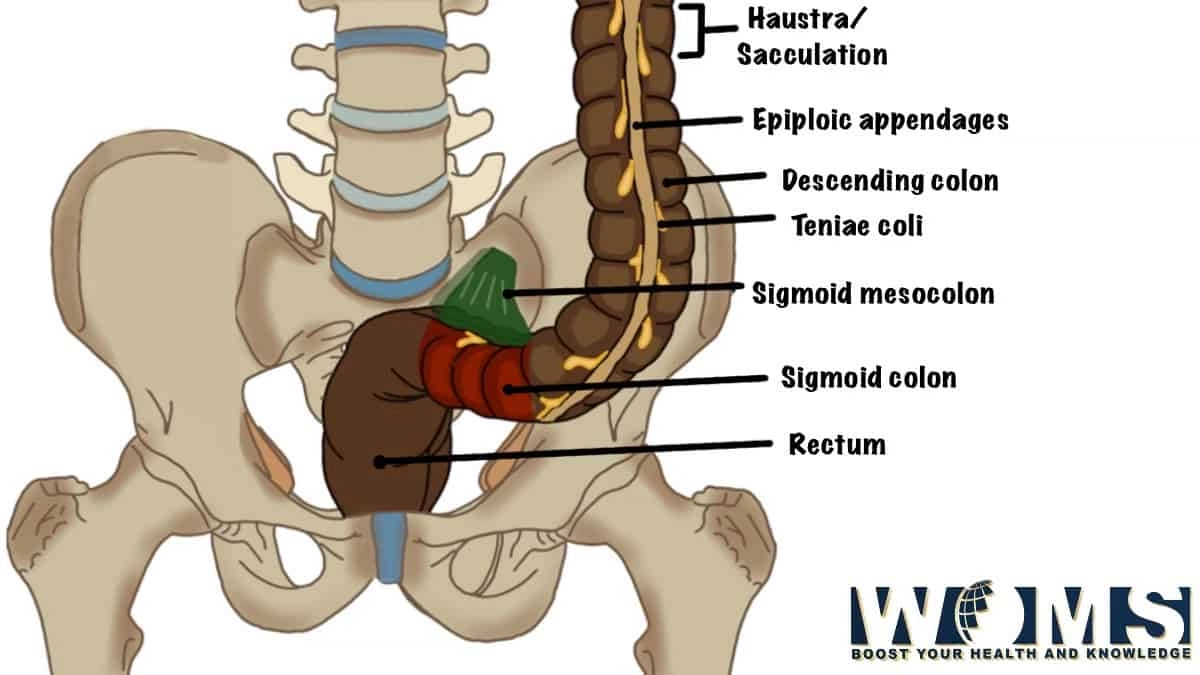
It starts from the pelvic brim continuing the descending colon. It turns back on itself descending into the pelvis. At this point, it is an intraperitoneal structure compared with the ascending and descending colon (retroperitoneal structures). It is covered with mesentery.
As the mesentery terminates, it is named as rectum. At this point, this colon becomes part of the rectum at a point of the 3rd sacral vertebrae. In contrast to the descending colon, a layer of peritoneum covers it. At the region of the 3rd sacral vertebrae, it again becomes a retroperitoneal structure just like the descending colon.
Function
The sigmoid colon offers a variety of functions being the gastrointestinal system. Let us have a detailed look at the functions to understand it better.
● The sigmoid colon works efficiently to excrete solid or gaseous waste products from the digestive tract. The curved shape of the sigmoid colon towards the anus enables the gaseous waste to collect in the superior curved portion. It helps the colon to excrete gaseous waste without excreting solid waste materials.
● It receives waste materials that may contain several nutrients and water. Its primary function is to reabsorb nutrients and water from the waste material at this point.
● It contacts through strong peristaltic waves to excrete the waste content present in it. Waste material from descending colon and sigmoid colon transfers to the rectum. Before the initiation of the defecation reflex, feces remain stored in the rectum for up to seven hours.
Sigmoid colon musculature
The sigmoid colon is motile due to the two layers of smooth muscles present within its walls. These layers contain an inner layer of circular muscle tissue with an outer longitudinal muscle tissue layer. In addition, longitudinal muscles form three visible muscle bands apparent on the external examination of the colon. These muscle bands are visible all around the sigmoid colon. It terminates at the rectosigmoid union.
These smooth muscle layers originate from the mesoderm layer. It works in the breakdown, condensation, and expelling of the waste materials to excrete from the rectum.
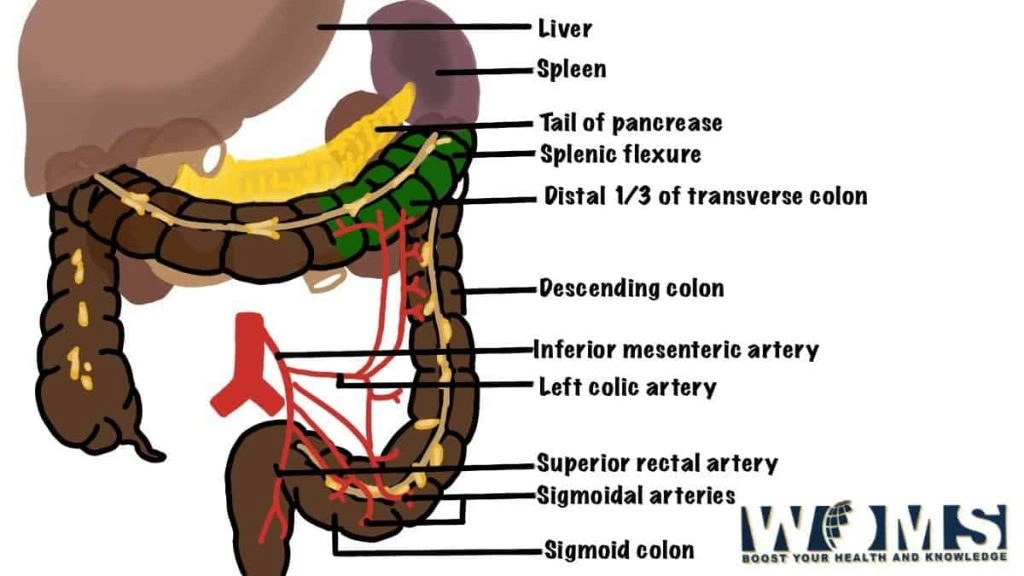
Blood supply of the sigmoid colon
The sigmoid colon develops from the hindgut. It receives its blood supply from the inferior mesenteric artery. More specifically, inferior mesenteric arteries divide into sigmoidal branches to provide blood supply. In addition, it also receives additional blood supply from the left colic artery superiorly and the rectal arteries inferiorly. Both of these arteries are the branches of the inferior mesenteric artery.
Lymphatic drainage
Lymphatic vessels follow the path of the inferior mesenteric arteries to drain lymph from the sigmoid colon. Lymphatic vessels bifurcate in a retrograde fashion to drain the lymph nodes in the mesentery. Ultimately, it terminates in the preaortic inferior mesenteric lymph nodes.
Nerve supply of the sigmoid colon
Gastrointestinal tract motility is under the maintenance of the enteric nervous system. The parasympathetic nerve supply of the sigmoid colon is through the pelvic splanchnic nerve from S2-S4. The cell bodies of the pelvic splanchnic nerves reside in the sacral parasympathetic nucleus. Moreover, its sympathetic nerve supply is through the lumbar splanchnic nerves from L1-L2. Lumbar splanchnic nerves communicate in the abdominal aortic and inferior mesenteric plexus.
The autonomic nervous system controls the activity of the enteric nervous system. This system develops as the neural crest cells originate from the ectoderm layer. It controls the motor and sensory neurons. There is a Meissner’s plexus in the submucosa. In addition, the Auerbach plexus is present between the longitudinal and circular smooth muscles of the gut. These plexuses control the activity of the gut essential for peristalsis.
Relations
Behind the sigmoid colon, there are the following important structures:
- External iliac vessels
- Ovary
- Obturator nerve
- Left piriformis
- Left sacral plexus of nerves
Whereas, the front of it is separated by coils of the small intestine from the bladder in males and the uterus in females.
Clinical aspects
Sigmoid colon secures prime clinical importance due to the part of the large intestine. There may arise several clinical complications to consider. Let us have a look at the clinical problems associated with it.
Hirschsprung’s disease
Hirschprung’s disease (aganglionosis) is associated with the contractility of the sigmoid colon caudally. In this condition, neural crest cells fail to migrate towards the distal colon. It may disturb the enteric nervous system. In this way, this disease affects the motility and normal function of the sigmoid colon. This condition is usually common in newborns with 5% of newborns with Down’s syndrome. The most common cause of this disease is mutations in genes.
Diverticulitis
A diverticulum is an out-pocketing of the wall of the large intestine. This condition most commonly occurs in the sigmoid colon. The common causes of diverticulitis are chronic constipation and a low fiber diet. If any fecalith is trapped in this out pocketing, it may get infected. Such patients present with a history of iliac fossa pain and blood in the feces. It is the most common condition in elders.
Sigmoid volvulus
Volvulus appears when the bowel twists on itself, constricting or closing the lumen. It occurs in people having a long sigmoid colon or mesocolon. This condition results in severe pain and absolute constipation. If this condition persists, oxygen perfusion decreases leading to ischemia and necrosis. Ultimately, peritonitis occurs.
Abdominal x-ray of such patients reveals coffee bean signs indicating volvulus. It is more common in children with rotation of the midgut. Treatment requires analgesia and immediate surgery.
Crohn’s colitis
It is an inflammatory bowel condition that can affect any part from the mouth to the rectum. The most common symptoms include diarrhea and weight loss with skin changes. This disease also manifests several extraintestinal symptoms like arthritis, erythema nodosum (purplish marks on legs), etc. Smoking may worsen the disease.
Ulcerative colitis
It is an autoimmune disorder with an inflammatory bowel condition. Earlier, it starts from the rectum and spreads proximally towards the gut. Symptoms are usually blood diarrhea with weight loss. It also includes multiple skin changes like anterior uveitis (inflammation of the anterior part of the eye), pyoderma gangrenosum (pustules on the skin of legs), and erythema nodosum. Unfortunately, smoking improves the disease.
Colon cancer
The malignant neoplasm may arise in the sigmoid colon. Usually, the neoplasm manifests itself with changes in bowel movements. It causes lower stool capability and hematochezia. Moreover, these colon neoplasms tend to metastasize to the liver using portal lymphatic drainage and lung via inferior vena cava.
Surgical importance
Surgeons can perform sigmoid hemicolectomy in case of recurrent diverticulitis or any malignancy. It is performed through the ligation of blood vessels, resection of the damaged colon, and creation of an anastomosis between the rectum and descending colon.
Surgeons may also perform sigmoid colectomy which is the complete removal of the sigmoid colon. It is usually done in patients with Crohn’s disease, bowel disease, or diverticulitis disease. After the complete resection, surgeons develop anastomosis between the rectum and descending colon to ensure the continuity of the large intestine.
What is sigmoid colon pain?
If you have an associated clinical condition, you might feel pain in the abdominal region. Nausea along with loss of appetite is also seen
Is sigmoidectomy a very painful process?
After undergoing the surgery, you might feel pain in the cut region of the colon. Moreover, flu-like symptoms may also be observed.
What causes inflammation in the sigmoid colon?
Inflammatory Bowel Disease may cause inflammation in the sigmoid colon. Besides this, obstruction in the blood supply to the colon and infections can also be the reason behind an inflamed colon.