A Comprehensive Guide to Posterior Cruciate Ligament
The posterior cruciate ligament is the robust and the greatest intra-articular ligament present in humans. It works in conjunction with its counterpart, the anterior cruciate ligament. In addition, this ligament maintains a communication of the posterior intercondylar aspect of the tibia to the medial condyle part of the femur. This orientation helps the posterior cruciate ligament to compromise on several forces that move the tibia in the posterior direction as compared to the femur.
The posterior cruciate ligament is intracapsular because of its presence deep within the knee joint. It is separated by the anterior cruciate ligament through a fluid-filled synovial cavity. Moreover, the synovial membrane covers these ligaments to absorb shock forces. This ligament gets its name due to its posterior orientation to the tibia. This article explains all the important anatomical aspects and clinical importance of the posterior cruciate ligament. Let us have a detailed look at the anatomical details of the posterior cruciate ligament.
Gross Anatomy of posterior cruciate ligament:
The posterior cruciate ligament surrounds the knee joint. There are several static or dynamic factors that provide proper stability to the knee joint to maintain function. It is considered an extra-synovial joint, properly surrounded by the synovial membrane. The overall length of this ligament at 90° flexion is about 32 to 38mm with an anteroposterior diameter of about 4.5 to 5.5mm. Whereas, the mediolateral diameter varies from 13 to 15 mm. In addition, it is twice as thick as the anterior cruciate ligament. The ligament consists of two main bundles to maintain the stability and integrity of the knee joint. Let us have a look at these two main bundles to know the anatomical features in detail.
Anterolateral bundle:
- It is about 65% substance of the posterior cruciate ligament.
- During flexion, the anterolateral bundle remains tight with the lax posteromedial bundle.
- This bundle performs the main function because of its increased cross-sectional area. Therefore, Surgeons usually prefer to reconstruct the anterolateral bundle of this ligament because of its more functional role.
Posteromedial bundle:
- It consists of about 35% of the total posterior cruciate ligament.
- During the extension of the knee, the posteromedial bundle remains tight with an anterolateral bundle in a lax position.
Attachments:
The posterior cruciate ligament is attached to different structures to maintain the integrity of the knee joint. Let us have a look at the internal attachments of this ligament to know from where it is starting or terminating.
Origin
The posterior cruciate ligament has its origin from the anterolateral surface of the medial femoral condyle present within the notch. From this point, it moves along the knee joint and continues to extend till its insertion.
Insertion:
The posterior cruciate ligament has its terminating point of insertion at the posterior surface of the tibial plateau. This point is approximately at a distance of 1cm, distally to the joint line. The Insertion points of the ligament are usually three times greater than the mid-substance.
Function of the posterior cruciate ligament:
The posterior cruciate ligament performs different stabilizing functions to maintain the performance of the knee joint. Let us have a detailed look at the different functions of this ligament. These are as follows:
- During the movements of the knee, the posterior cruciate ligament moves in a way that the anterolateral part stretches in the direction of flexed knee preventing knee extension. In the same way, the posterolateral aspect of this ligament stretches in the knee extension.
- The main purpose of this ligament is to maintain the stability of the femur to move away from the edge of the tibia.
- In addition, it also helps to maintain the stability of the tibia by moving away from the femur bone.
- Moreover, this ligament works as a whole to prevent the translation of the femur over the tibia anteriorly.
- During the flexion and maintaining weight on the knee, the posterior cruciate ligament stabilizes the femur.
- Besides stabilizing features, the posterior cruciate ligament also helps maintain a connection between the tibia and femur.
Biomechanics:
The posterior cruciate ligament is the main ligament for the translation of the tibia posteriorly. Its function is more prominent during deeper flexion. Any posterior displacement of the tibia beyond 10mm indicates a complex injury of this ligament in combination with posterolateral ligamentous structures. This ligament also stabilizes the knee secondarily to maintain knee flexion between 90° to 120° to prevent any excessive rotation.
The biomechanics of the ligament lies in the independent functioning of the two bundles. The anterolateral bundle works during knee flexion. Whereas, the posteromedial bundle works during knee extension. These two bundles usually work synergistically to maintain the performance of the ligament.
Different studies suggest that any injury that may tear any of the bundles can cause dysfunction of the knee joint. Any injury may not be able to produce an adequate posterior translation of the tibia. Moreover, any isolated rupture of the posterior cruciate ligament produces a significant effect on knee flexion at 90°. Therefore, the maintenance of this ligament is diagnosed at 90° knee flexion.
In addition, during knee flexion, anterolateral bundles of the posterior cruciate ligament are tightened with the posteromedial bundle in the lax position. The opposite happens during the knee extension.
The majority of the strength is provided by the Anterolateral bundles of this ligament with a tensile strength of 1620N. Whereas, the tensile strength of the posteromedial bundles of the ligament is 258N. This difference in tensile strength is mainly due to the cross-sectional area of these two bundles.
Vascular supply:
Every structure owns its blood supply to maintain perfusion. The posterior cruciate ligament receives its blood supply through the middle genicular artery. This artery breaches the posterior capsule of the joint moving parallel to the upper aspect of the synovial septum. At this, it delivers its branches to the synovium encircling the ligament. It forms a plexus of vessels that supply the posterior cruciate ligament. In addition, it also receives additional blood supply through the inferior genicular artery.
Nerve supply:
Ligaments receive their nerve supply following Hilton’s Law. It dictates that a joint is innervated by the same nerves of the muscles that cross the joint. Following this, the tibial and obturator nerve deliver posterior articular branches to the posterior capsule. These branches perforate the posterior capsule to approach the posterior cruciate ligament.
Clinical significance of the posterior cruciate ligament:
The posterior cruciate ligament is the main stabilizing factor of the knee joint. There are two common types of pathologies associated with this ligament. These are as follows:
- Posterior cruciate ligament tear
- Double posterior cruciate ligament sign
- Posterior cruciate ligament tear:
Posterior cruciate ligament tears count for 3% of outdoor patients with ligament years and 38% of patients suffering from acute traumatic knee hemarthrosis. These injuries may happen separately. But, in 95% of cases, these tear injuries happen in combination. The ligament tears are associated with increased morbidity with decreased function. Because it causes continuous instability with pain, dysfunction, and progression into degenerative joint disease.
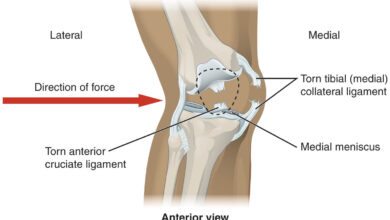
These tears are usually caused by external forces like dashboard injury due to force directed in the posterior direction but on the anterior surface of the proximal tibia with knee flexion. Symptoms are usually variable depending on the injury mechanism. Stiffness, tenderness, and swelling of the posterior region of the knee are the classical symptoms. Moreover, pain in the anterior knee or instability while descending stairs indicates chronic isolated tears.
You should check out these Essential facts about pain behind knee.
Diagnostic tests:
A careful clinical examination is mandatory to assess the injury associated with the popliteal artery. Acute posterior cruciate ligament injuries exhibit typical symptoms of swelling and restriction of 10 to 20° flexion due to pain. Whereas, chronic injuries present with restricted activities like difficulty in climbing slopes due to pain and lethargy in the anterior and medial aspects of the knee.
The most important and accurate diagnostic test for this ligament is the posterior drawer test. At 90° knee flexion, there is sagging of the tibia posteriorly on the injured side. If the tibia is pulled forward or the quadriceps contracted at 90° knee flexion, there is an instability of the knee anteroposteriorly.
Proper physiotherapy management is essential to deal with such kinds of injuries.
Double posterior cruciate ligament sign:
The double posterior ligament sign is visible on the sagittal MRI of the knee. It appears when a bucket-handle meniscal tear moves towards the center of the knee joint. It comes to approach the anteroinferior aspect of the posterior cruciate ligament to mimic a smaller ligament. There are several symptoms associated with this condition. Some of them are as follows:
- Central meniscal part
- Missing bow tie sign
- Sign of fragment-in-notch
- Displaced meniscus
Conclusion:
The posterior cruciate ligament plays a prominent role in the complex anatomic structure of the knee joint. Together with other ligaments of the knee, it maintains the stability and clinical performance of the knee. The posterior cruciate ligament consists of two main bundles maintaining the stability of the knee. There is a high need to remember the anatomical features of this ligament to know the kinematics and reconstruct the ligament. It helps to understand the importance of this ligament for conservative or surgical procedures on the knee joint.
Frequently asked questions (FAQs)
How can we diagnose an injury to the posterior cruciate ligament?
There are several ways to inspect the injury of the posterior cruciate ligament. Your doctor may clinically examine your knee by estimating the extent of movement of your knee. In addition, there are several symptoms suggestive of any injury associated with the posterior cruciate ligament. Moreover, there are several other diagnostic tests to confirm your clinical findings. These are as follows:
● Radiographic findings through X-rays
● Magnetic resonance imaging to determine soft tissue or ligament tear
● Computerized tomography scan
How can we treat the injuries of the posterior cruciate ligament?
There are several management plans for the posterior cruciate ligament injury depending on the severity of the damage. The most common treatment regimens are as follows:
● Crutches to limit the weight in the knee.
● Knee braces to normalize knee instability.
● Physical therapy through exercise helps to strengthen and stabilize the knee joint.
● Surgical procedures to treat aggressive injuries
How long does it take to heal a posterior cruciate ligament injury?
The healing period varies from one person to another person. Mild injuries may heal up to 10 days in a healthy person. Whereas, in case of severe injuries, it may take six to nine months to heal properly.