Normal as well as variant anatomy of the dural venous sinuses
The anatomical diversity in the dural venous sinuses is significant. The practicing neuroradiologist must have a thorough understanding of dural venous sinus architecture and typical anatomic variations to distinguish between normal and pathologic situations.
We use an image-based method to evaluate dural venous sinus architecture as well as highlight frequent variations in this study.
Introduction of Dural venous sinuses
The intracranial venous system, most specifically, the dural venous sinuses, demonstrates considerable anatomic variation. Neuro-radiologists should be familiar with common variants to make accurate diagnoses as well as avoid misdiagnosis.
Firm knowledge of DVS anatomic variations may also prove useful during preoperative evaluation. Herein, we review normal DVS anatomy, with an emphasis on common anatomic variations.
Normal intracranial venous anatomy as well as its variant
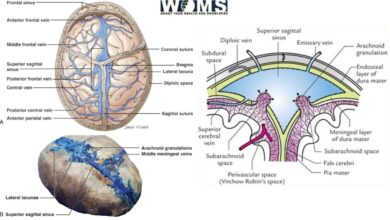
The intracranial venous system comprises the superficial cerebral veins, the dural venous sinuses, as well as the deep venous system (Figure 1).
It is surrounded by dura mater, like the superior sagittal sinus (SSS), inferior and straight sinus, the conflux of the sinuses (Torcular Herophili), transverse sinuses, and sigmoid sinuses.
The deep venous system drains profound white matter (WM) and grey matter (GM) structures, which includes the internal cerebral veins, the basal veins of Rosenthal, and the great cerebral vein of Galen. The superior and inferior petrosal sinuses facilitate drainage between the DVS and cavernous sinus complexes.
The spheno-parietal sinus drains medially into the cavernous sinus and is found under the lesser wing of the sphenoid. This sinus connects into a subdivision of the middle meningeal vein and runs in a vascular groove along the floor of the middle cranial fossa, with additional contributions from the orbit, temporal uncus, and inferior frontal veins.
The occipital sinus is the smallest DVS, is intra-dural, and has been studied the least. It is a single or paired midline venous structure, either arising from the Torcular Herophili or the medial transverse sinus. These are draining into the confluence of the marginal sinuses, which then empties into the jugular bulbs.
The marginal sinus is found with the boundary of the foramen magnum, and communicates anteriorly with the basilar venous plexus and posteriorly with the occipital sinus. It typically drains into the sigmoid sinus.
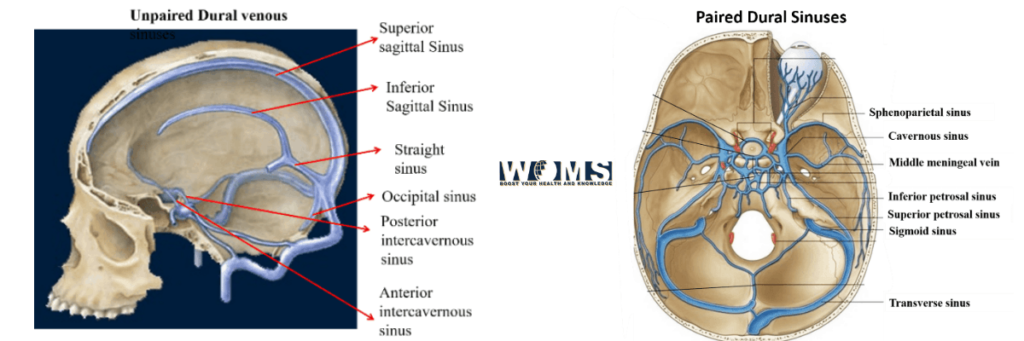
There are many ways to classify the DVS. A few salient ones are tabulated as follows:
Unpaired
- Intercavernous sinus
- Occipital sinus
- Inferior sagittal sinus
- Straight sinus
- Superior sagittal sinus
Paired
- Intermediate anastomotic veins
- Spheno-parietal sinus
- Inferior petrosal sinus
- Cavernous sinus
- Sigmoid sinus
- Superior petrosal sinus
- Basilar venous plexus
- Transverse sinus
The 4 important anastomotic veins are:
- Sylvius (Sylvian) vein
- Vein of Rolando
- Vein of Labbé
- Vein of Trolard
Superior sagittal sinus(SSS)
The most popular change of the SSS is the abnormality of its rostral end. The variations of the rostral end of the SSS :
- Type1, a fully mature rostral SSS;
- Type 2, the duplicate of the rostral SSS, with bilateral Hemi- Superior sagittal sinus;
- Type3, complete hypoplasia of the rostral SSS, with bilateral parasagittal superior frontal veins; as well as
- Type4, a unilateral Hemi- Superior sagittal sinus, with an unpleasant contralateral parasagittal superior frontal vein.
Inferior Sagittal Sinus
Congenital lack of the inferior sagittal sinus is a common convergence variance, and, in single research, it was shown that it was absent in 13.95%of the patients. The inferior sagittal sinus may have a non-classic point of origin or termination.
For example, the inferior sagittal sinus may be emptying into the SSS rather than into the straight sinus. It is often more pronounced on imaging in infants as well as children compared with adults.
Torcular Herophili and Straight Sinus
Considerable anatomic variation exists at the Torcular Herophili, as well as various classification systems have been proposed. The number of classification systems for the Torcular Herophili reflects its considerable anatomic variance.
One classification system for the Torcular Herophili, which has 3 types;
- In type 1, the SSS empties into a transverse sinus and the straight sinus drains into another transverse sinus, with no relation between the 2-independent circuits.
- In type 2, both the SSS and the straight sinus bifurcate or divide prematurely, and the branches from the SSS and straight sinus join to form a transverse sinus on each side.
- In type 3, a “confluence of sinuses” was observed. Various subtypes exist within type 3 because this “confluence of sinuses” could refer to anything, varying from the classic Torcular Herophili (a “common pool”) to a “potential confluence” (due to the existence of a dural pad, a partial dural partition, or a complete dural partition).
The drainage structure of the Superior sagittal sinus into the transverse sinuses into 4-types:
- Type Sc, the classic anatomy where it drains into a true confluence;
- Type Sd, it untimely dividing into the right as well as left limbs as well as emptying into the same-sided transverse sinus;
- Type Sr, where it is emptying into the right transverse sinus; as well as
- Type SI, where it preferentially emptying into the left transverse sinus.
The 3 types of Torcular Herophili:
- Type 1, a true confluence;
- Type 2, a partial confluence; as well as
- Type 3, a non-confluence.
Anatomic variations exist is at the confluence of the vein of Galen and straight sinus, with important implications for pineal region surgeries.
In one study, the basal vein of Rosenthal described 4 patterns of drainage:
- Type-1, emptying into the internal cerebral veins;
- Type-2, draining at the connection of the internal cerebral veins;
- Type-3, emptying into the vein of Galen; as well as
- Type-4, emptying into the straight sinus.
The type 0 variant indicates the absence of a basal vein of Rosenthal. The type 3 variant was the most commons.
Transverse as well as Sigmoid Sinuses
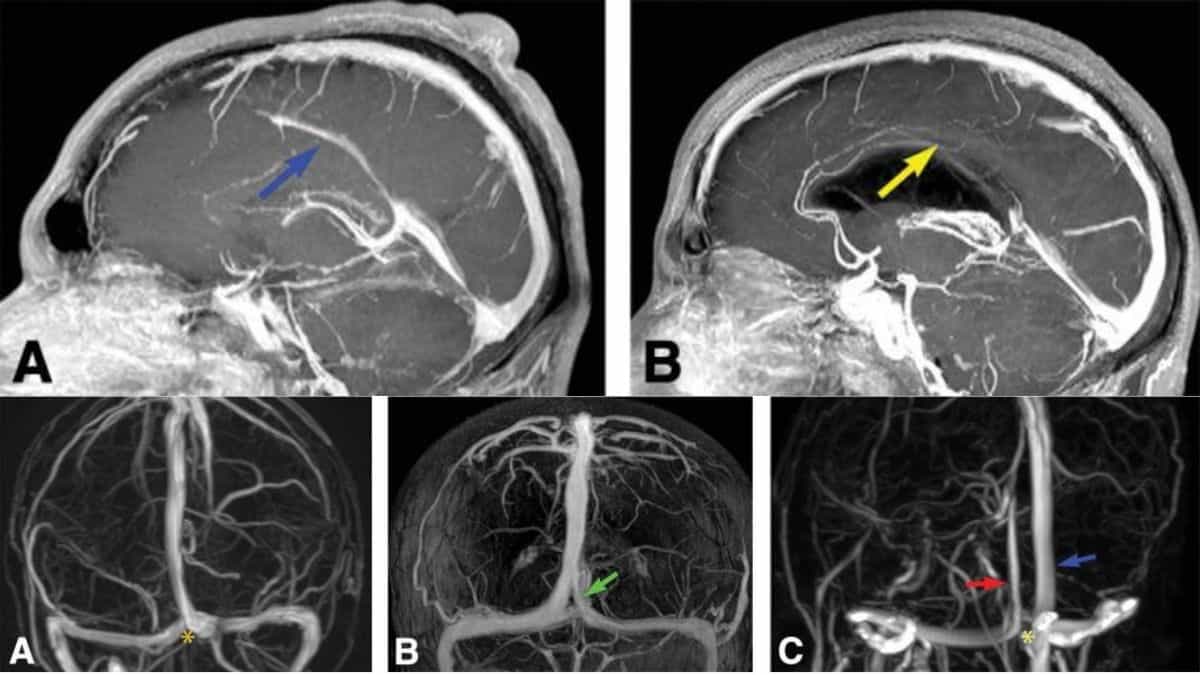
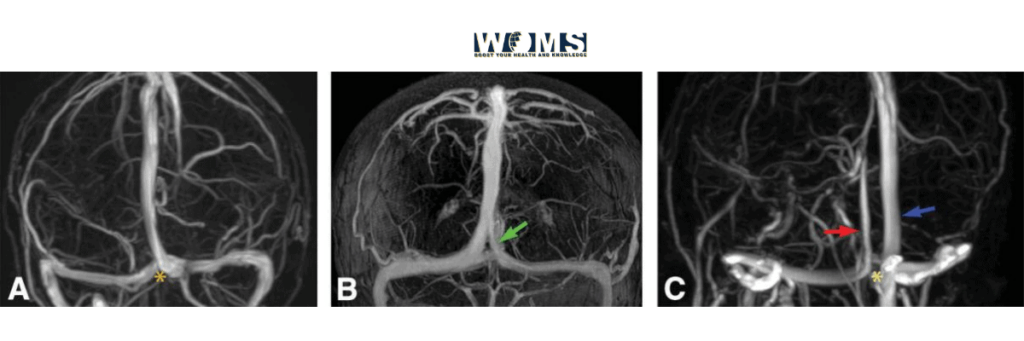
Co-dominance of the transverse sinuses is typically the most frequently encountered appearance of the transverse sinuses (Fig-5A). A common variant of the transfer sinuses is asymmetry (unilateral dominance)(Fig-5B). When asymmetry of the transverse sinus is present, it is most popular for the rights sinus to be dominant.
A study found the left transverse sinus was10times more likely to be hypo-plastic than the right transverse sinus. When unilateral dominance of the transverse sinus occurs, the Superior sagittal sinus will typically empty into the dominant transverse sinus and the no dominant transverse sinus will empty the straight sinus.
It is also possible for one transverse sinus to be congenitally absent. In transverses sinus atresia, the ipsilateral sigmoid sinus often receives drainage directly from the vein of Labbe. The sigmoid sinuses may be asymmetric in size or there can be unilateral absence. In one study, a hypoplastic sigmoid sinus existed in 25% of pts and anaplastic sigmoid sinus was present in 0.98% of pts. A unilateral congenital absence of the sigmoid sinus may be accompanied by a large Torcular Herophili.
Occipital Sinus
The occipital sinus was previously established to be present in approximately 57.5% of adults. In another study, was present in approximately 18% of pediatric patients. Studies with pediatric patients demonstrated a decreased prevalence of the occipital sinus with age.
Several studies in pediatric patients demonstrated a decreased prevalence of the occipital sinus with age. More commonly present in patients <2 years old as well as absent inpatients>9 years of age.
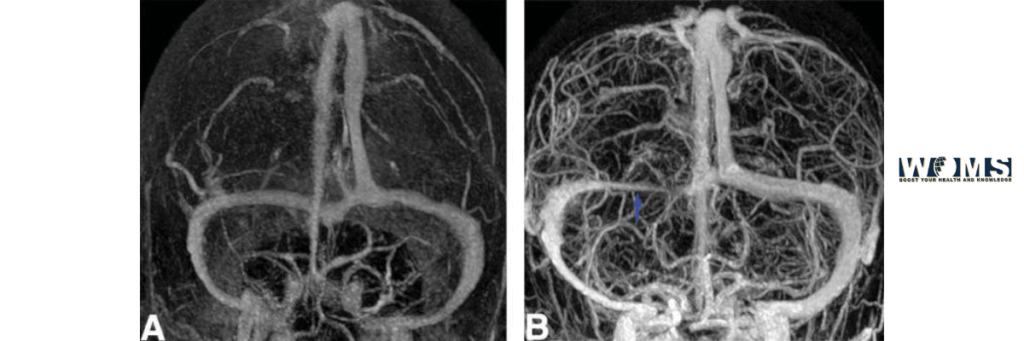
The greater prevalence of the occipital sinus at younger ages suggests that it may involute with time. Classically, the occipital sinus is a single midline structure (Fig 6A, B). It may be diverted to one side, more commonly toward the right.
The occipital sinus empties into the confluence of the marginal sinuses, which eventually drain into the jugular bulbs. The “oblique occipital sinus” is a common variant, which deviates from the midline and typically drains into the internal jugular vein or sigmoid sinus (Fig 6 C, D).
This variant has surgical implications for posterior cranial fossa surgeries. Bilateral occipital sinuses are an anatomic variant associated with duplicated falx cerebelli.

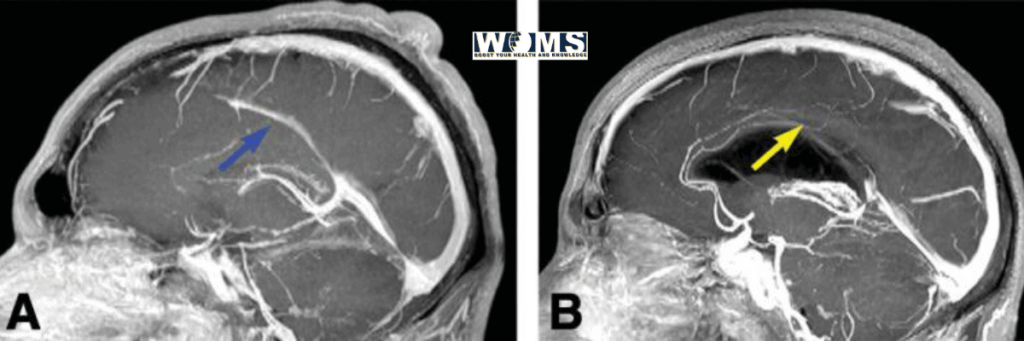
Falcine Sinus
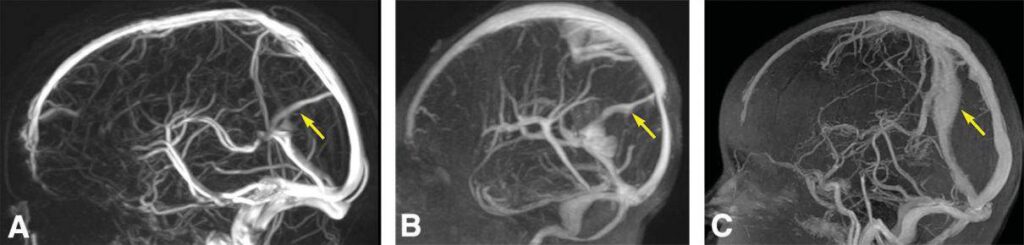
The falcine sinus connects the vein of Galen with the Superior sagittal sinus throughout fetal life. It normally involutes after birth but can be observed in children as well as adults (fig-7). The falcine sinus may connect the inferior sagittal sinus to the SSS, rather than the vein of Galen to the SSS.
The falcine sinus may be duplicated. A falcine sinus can be connected with inborn abnormalities, like a vein of Galen abnormality, parietal or occipital encephaloceles, lack of the corpus callosum, and a dysplastic tentorium, and with stenosis or occlusion of the Superior sagittal sinus or straight sinus, or with the absence of the straight sinus. A falcine sinus has also been observed in the setting of DVS thrombosis.
However, a falcine sinus has also been observed without any associated congenital anomalies or sinus occlusion, stenosis, or absence. This suggests that there are 2 distinct pathogeneses for a falcine sinus observed after birth: either the falcine sinus never in volute after its formation during the fetal period (referred to as a“persistent falcine sinus”) or a falcine sinusinitially involute during the fetal period as well as then recanalize data later point in life due to an inciting event, such as venous thrombosis.
Drainage of the Dural Venous Sinuses
The DVS complex is a massive network of venous aqueducts that allows for efficient venous circulation from the brain to the internal jugular veins.